Page Contents
How current was the study?
The study was published on June 19, 2021 on the medRxiv website. Their about page states: “medRxiv (pronounced “med-archive”) is a free online archive and distribution server for complete but unpublished manuscripts (preprints) in the medical, clinical, and related health sciences”.
The purpose of the study was to “evaluate the necessity of COVID-19 vaccination in persons previously infected with SARS-CoV-2.” The article continues,
“the CDC website recommends that persons previously infected with SARS-CoV-2 still get the vaccine [10]. Despite these recommendations, credible reports of previously infected persons getting COVID-19 are rare. The rationale often provided… is that it is safer to get vaccinated than to get the disease. This is certainly true, but it is not an explanation for why people who have already had the disease need to be vaccinated. A strong case for vaccinating previously infected persons can be made if it can be shown that previously infected persons who are vaccinated have a lower incidence of COVID-19 than previously infected persons who did not receive the vaccine.”
Introduction, Para 3.
Is there a source?
The source publication for this study can be found here. In addition, the researchers also made the dataset available publicly, including the code to reproduce the results. That can be found here.
Citation
Shrestha N, Burke P, Nowacki A, Terpulek P, Gordon M.Brown. Necessity of COVID-19 vaccination in previously infected individuals, June 2021. medrxiv 2021. DOI: https://doi/10.1101/2021.06.01.21258176
Primary or Secondary Dataset?
This study was based off of a Primary Dataset with appropriate approvals from Cleveland Clinic’s Institutional Review Board (IRB).
How was the sample collected?
According to the article, “Employees of the Cleveland Clinic Health System working in Ohio on December 16, 2020, the day COVID-19 vaccination was started, were included.” So basically all 52,238 employees were included, which is an interesting aspect of this study. Remember, the sample of a study is intended to represent some larger group of people. This is a very large sample, with a very diverse range of demographics, socio-economic factors, and health backgrounds. It is limited to healthcare employees in Ohio. I don’t have information on these factors, so I would be careful to extrapolate the outcomes of this study to children or to the elderly. It also may not be representative of other geographies, countries, or cultures.
Here are some of the variables mentioned in the study.
- Previously Infected – SARS-CoV-2 infection (in other words someone already had COVID) was determined by a positive nucleic acid amplification test (NAAT) 42 days prior to the vaccine rollout date. See the note below on why 42 days.
- Date of Infection – was considered the date symptoms appeared or the date a specimen was collected if there were no symptoms.
- Fully Vaccinated or Vaccinated – Persons were considered vaccinated 14 days after receiving the second dose of the vaccine.
- Time to SARS-CoV-2 Infection – the number of days from December 16, 2020, when the vaccine was rolled-out, to the date of a positive NAAT test for SARS-CoV-2.
- Additional variables included:
- Age
- Job Location
- Job Type (patient-facing or non patient-facing)
- Job Category.
In addition to these variables, also of note is that the screening for COVID was based on suspicious symptoms and/or right before medical operations and procedures. They did not regularly screen employees that were asymptomatic (symptom-less). So it’s possible there were additional COVID infections in the employee population that were not identified.
Why 42 days?
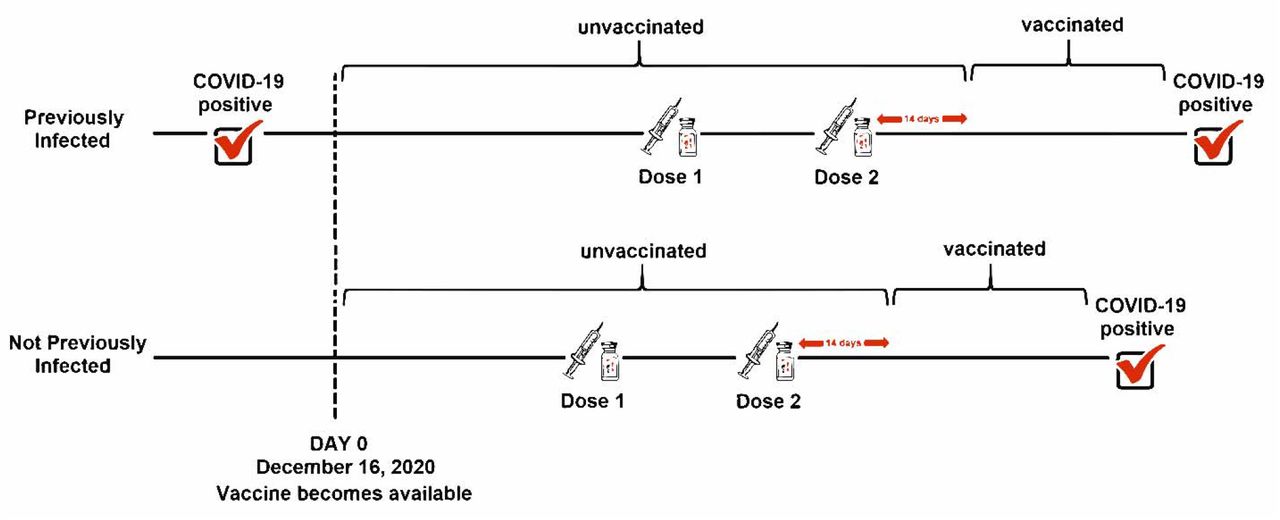
The researchers wanted to compare natural immunity to vaccinated immunity. They determined a previous infection as someone who had a positive COVID test 42 days prior to the vaccine rollout date, because that’s the length of time they calculated for vaccinated immunity. So how did they calculate vaccinated immunity? In most cases, the first dose of the vaccine was 28 days prior to the second dose of the vaccine, and then 14 days after that persons were considered fully vaccinated. So the timespan from Dose 1 through Dose 2, and 14 days later, was approximately 42 days.
What were the findings?
The researchers used a Simon-Makuch hazard plot to compare the total number of COVID infections among:
- previously infected persons who were vaccinated
- previously infected persons who were remained unvaccinated
- previously uninfected persons who were vaccinated
- previously uninfected persons who remained unvaccinated
Remember, “previously infected” are people who had COVID at least 42 days before December 16, 2020, and “vaccination” refers to 14 days after receipt of the second dose of a vaccine.
The article describes how persons moved from the unvaccinated status to the vaccinated status. You can read it if you’d like or look at the following graphic. I think it does a good job of showing how people who were previously infected or previously uninfected moved from unvaccinated to vaccinated.
So here’s some stats:
- 2,579 (5%) of the 52,238 employees were previously infected with COVID.
- Previously infected persons were younger on average, (39 years) than previously uninfected persons (42 years).
- Previously infected persons had a significantly higher proportion of patient facing jobs (65%) than previously uninfected persons (51%).
Here’s the source with a breakdown of the variables that I think you’ll find helpful. For your convenience I’ve included it here. You can see that the majority of the previously infected cases were nurses, 1,142.
Below is a comparison between previously infected and previously uninfected persons who were vaccinated during the study:
- 1,220 (47%) of the 2,579 previously infected persons were vaccinated before the end of the study.
- 28,855 (58%) of the previously uninfected persons were vaccinated before the end of the study.
Some additional stats:
- 63% of people vaccinated received the Moderna vaccine.
- 37% received the Pfizer vaccine. (Inferred based on the introduction to the study. I didn’t see this specifically called out.
- 12% of the previously infected did not have a symptom onset date, which suggests that they likely tested positive due to an upcoming medical operation or procedure.
- The vaccination roll-out happened at the peak of the third wave of the epidemic in Ohio.
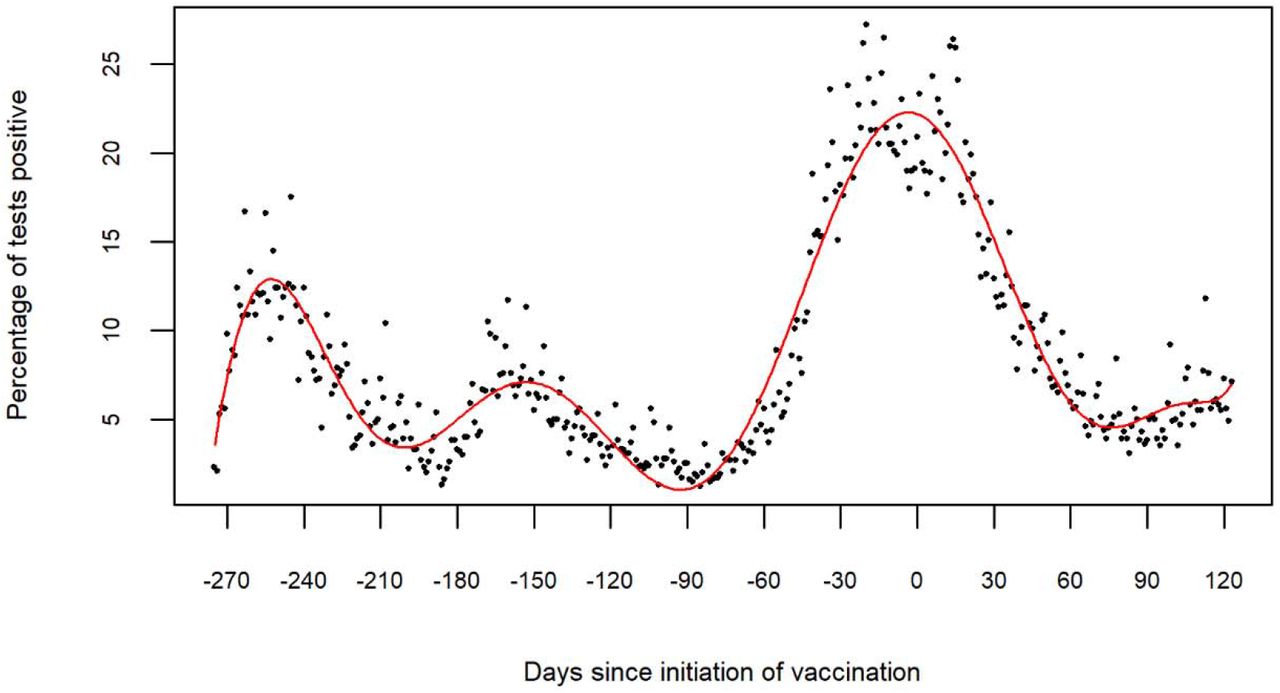
Figure 2, above, shows the 270 days prior to December 16th, to 120 days after December 16th. The Highest peak above the zero (0) – or (“zed” mark for my European friends) represents December 16th, 2020.
The last figure, below, is of the Simon-Makuch plot.
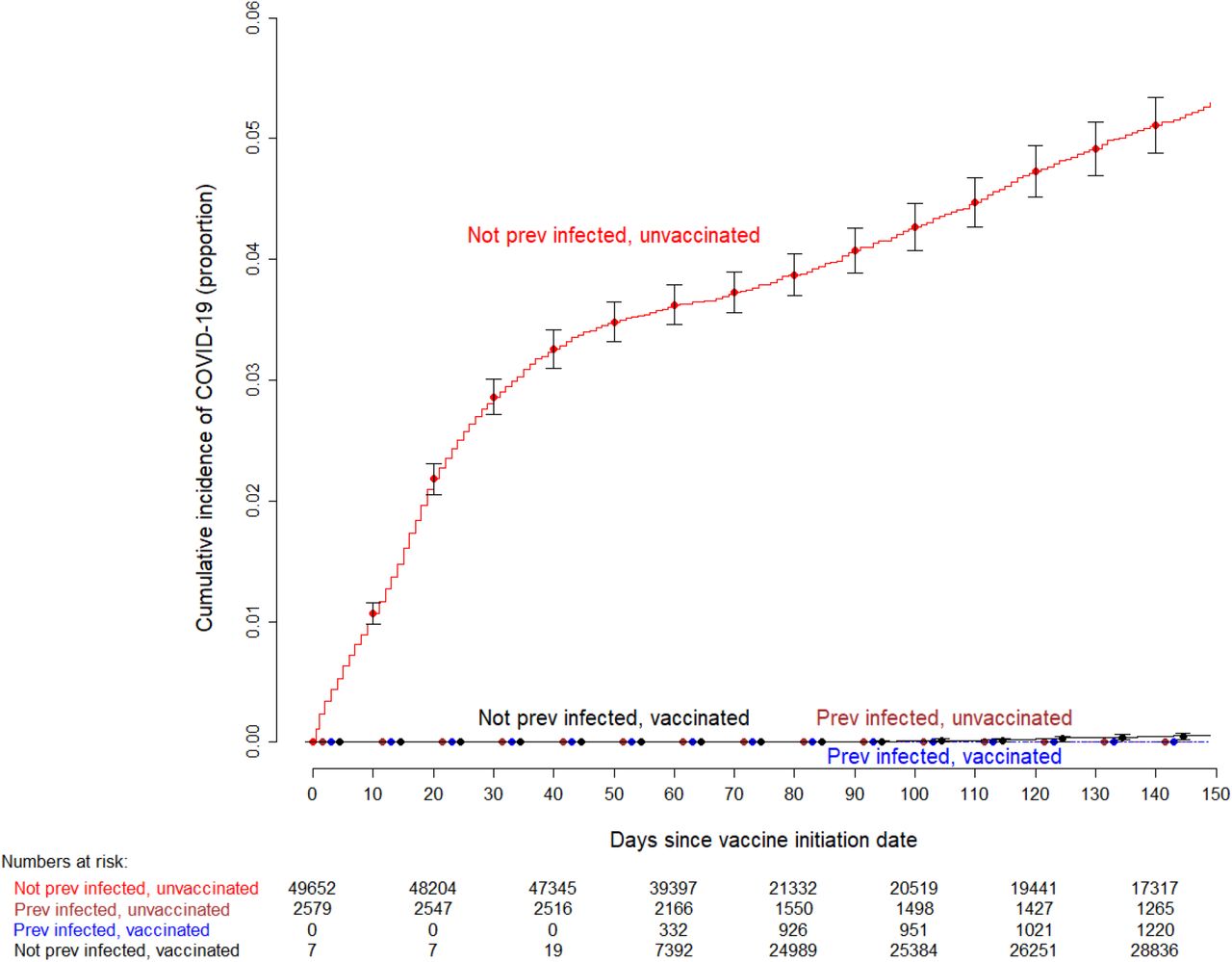
The red line that climbs high is the cumulative number of COVID infections (proportionally) over time for people who were not previously infected and who were unvaccinated. By far the most instances of infection happened here.
Notice the pink and blue lines, previously infected, unvaccinated, and previously infected, vaccinated. See how they remain flat? If antibodies from previous infections did not protect against future infection, then we’d likely see that previous infected, unvaccinated rate climb. But it doesn’t. It stays consistent with the previously infected vaccinated.
Also notice the black line – not previously infected, vaccinated. It doesn’t climb either, indicating that the vaccination prevented infections as well as antibodies from a previous infection. There is no significant difference.
The study states what I just wrote:
“SARS-CoV-2 infections occurred almost exclusively in subjects who were not previously infected with SARS-CoV-2, and who remained unvaccinated. The cumulative incidence of SARS-CoV-2 infection among previously infected unvaccinated subjects did not differ from that of previously infected subjects who were vaccinated, and that of previously infected subjects who were vaccinated”
Section: Cumulative incidence of COVID-19. Paragraph 1.
To be more specific:
- 2,139 (99.3%) of the 2,154 infections occurred among people who were not previously infected and who remained unvaccinated.
- 15 (0.7%) of the 2,154 infections occurred among people who were not previously infected who were vaccinated.
- Not one of the 2,579 previously infected subjects had a SARS-CoV-2 infection, including the 1,359 who remained unvaccinated.
For those who have had COVID, that last bullet point should stick out to you. According to this study, if you’ve had COVID, and the sample included in the study is representative of you, that should give you a bit of peace of mind. Now keep in mind, this study is not about the Delta variant. That’s a different discussion altogether, though.
The article also states that the study wasn’t intended to showcase the duration of protection provided by natural immunity. Based on the timing of the study, the researchers inferred that a COVID infection may provide protection against reinfection for 10 months or longer.
By the way, if you want to get your antibodies tested, you can do so through organizations like Quest Diagnostics. It’s a quick blood draw and results are provided electronically within a couple of business days. I just had mine tested and it was ~$150. If you were wondering, my 9 month old antibodies are looking as great as ever. 🙂
What does the study show?
Persons previously infected with COVID are unlikely to get reinfected regardless of the vaccine. “this finding calls into question the necessity to vaccinate those who have already had SARS-CoV-2 infection.”
“Reports of true reinfections are extremely rare in the absence of emergence of new variants. When such reinfections occur, it would be purely speculative to suggest that a vaccine might have prevented them. Duration of protective immunity from natural infection is not known. However, the same also can be said about duration of protective immunity from vaccination. Uncertainty about the duration of protective immunity afforded by natural infection is not by itself a valid argument for vaccinating previously infected individuals….This study provides direct evidence that vaccination with the best available vaccines does not provide additional protection in previously infected individuals.”
Section: Discussion, paragraph 2.
The very next paragraph in the discussion cites prior studies that showed contrary outcomes, and then describes why this study is a more appropriate determination. This post is already long enough, so I’ll let you read that for yourself if you’d like.
What were the limitations?
The study actually cited it’s strengths first.
- Large sample size
- 5 month follow-up
- Adjustment of the analyses based on the phase of the epidemic
- Health system study with policies and procedures recognizing the critical importance of the study including collection of information.
The study also cited limitations.
- There was not a policy to test for asymptomatic employees. So previously uninfected persons could have actually been infected, and then reinfected.
- The follow-up duration was short, only 5 months, but longer than mRNA vaccine efficacy studies, and longer than the follow-up duration of the largest published vaccine effectiveness studies to date.
- The study included no children and few elderly and the majority would not have been immunosuppressed.
- Data governance prohibited getting additional clinical information on employees.
- The study is based on the variants of COVID 19 prevalent in the community during the study. So different variants could have different results. “If prior infection does not afford protection against some of the newer variants of concern, there is little reason to suppose that the currently available vaccines would either. Vaccine breakthrough infections with variants have indeed been reported.”
The study concludes with a statement suggesting previously infected individuals are unlikely to benefit from COVID-19 vaccination.
What you should consider
- Did they cite a source and can you navigate to it? 10/10. You can go download the source yourself.
- Did the source clearly describe how the data was acquired. 7/10. They left a lot for inference. It was an internal study at the Cleveland Clinic, but they didn’t go into much detail on the systems the data were contained in.
- Did the source cite potential biases or limitations to the study? 8/10. They had a pretty robust study. I felt like their list of weaknesses were represented as strengths almost – like an interview candidate picking picking one of their strengths as a weakness. 🙂
- Is the source reputable? 10/10. The Cleveland Clinic is a world-renown healthcare organization.
- We’re there enough participants in the sample? 9/10. The sample size has an N > 32, which is often the threshold to meet statistical significance. There were over 50,000 people included in this study. Limitations cited were that there were no children or elderly. It also didn’t go into detail on other demographics. The sample size, though, is a very large study. Actually, larger than the sample used for FDA approval of the Pfizer vaccine.
- Did the study or news article focus on one finding and not talk about other findings that are obviously visible in the study? 10/10. I feel like this is an underrepresented study in the news. I didn’t notice other details that I thought were significant. This was a more complex study to breakdown, though, so it’s possible I was too fatigued to notice.
- Are all the variables included that you think are necessary to arrive at the same conclusion, or at least identified as limitations? 8/10. I would have liked more demographic variables in the study (i.e. race, gender, age, etc…) in order to better define the population the sample represents. I do think it’s intriguing that a large portion of the previously infected were nurses. I’m curious how many of them were vaccinated or not. These are front-line workers exposed directly and frequently to infected patients.
- Is the study clearly described to the point that it could be reproduced by someone else given the same data and research background? 7/10. In my opinion, they didn’t do a great job describing the collection mechanisms for the study. The types of statistical analyses were described, including any censoring of the data.
My Conclusion
Based on this study, people who have had COVID and have not been vaccinated do not benefit from being vaccinated. The media or medical professionals who suggest that the vaccine protects more against variants than natural immunity are speculating at best. I am looking for a study that shows otherwise, so please share it with me if you know of one. Please note, there are a few studies that this research cites, that indirectly suggest otherwise, and this study explains why this is a better study.
Also based on this study, people who have not had COVID, do benefit from the vaccine in terms of protection against the virus itself. There are studies out of Israel, with likely the highest vaccination rates of any nation, that suggest breakthrough infections (infections after vaccination) are rampant. I’m planning to review one of those studies next.
If you are an employer navigating vaccination policy decisions for your team, Leaders Eat Last (#ad) by Simon Sinek is a good read on putting your people first.
**One thing I also want to note, is that I’m not a physician, and I am not giving medical advice. I’m just sharing my thoughts on what this study shows. You look at the data, and determine for yourself what medical care is right for you. It’s not up to your employer, or your government. You make the decision one way or the other, because in the end, you are the one who has to live (or not live) with the results.
Working through this with your team?
This is exactly what we do at Stephens Insight Group helping organizations develop leaders, build strategy, and fix culture.
Talk to us about your organization